|
|
Rheumatoid Nodules of the Lung
Necrobiotic Nodules
General Considerations
- Rare
- Immune-mediated granulomas frequently with necrotic centers
- They are almost always associated with long, standing active rheumatoid arthritis
- More frequent in males with high titers for rheumatoid factor
- Also more frequent in smokers and those who already have subcutaneous nodules
- Rheumatoid nodules are most common subcutaneously
- They may also occur in the lungs, heart and trachea
- Incidence on chest x-ray in RA is less than 1%
- Using CT, their incidence increases to 22-28%
Clinical Findings
- Mostly asymptomatic
- Sometimes cough
- Hemoptysis
- Chest pain
Imaging Findings
- Rounded, multiple, subpleural
- Rarely solitary
- Middle and upper lung zones more common, except with Caplan Syndrome (with pneumoconiosis)
- Up to 50% cavitate, frequently apical lesions, usually thick-walled with smooth inner margins
- Cavities may then harbor aspergillosis
- Also associated with pleural effusion and/or pneumothorax and bronchopleural fistula
- Rarely calcify
Differential Diagnosis
- Metastases
- Granulomatosis with polyangiitis (Wegener’s)
- Septic emboli
Treatment
- Do not require a specific treatment
- Intervention only when a complication occurs
- Nodules may respond to methotrexate and/or steroids
Prognosis
- May regress without treatment
- Nodules may follow course of arthritis or behave independent of its course


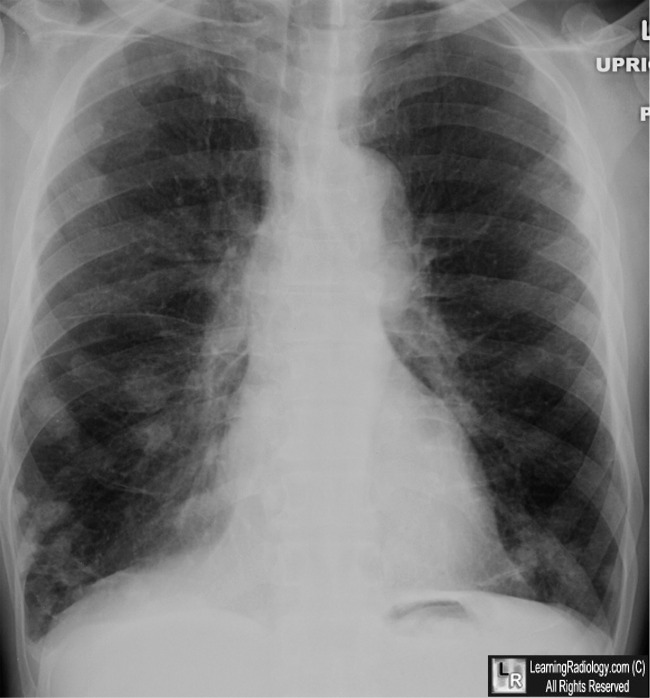
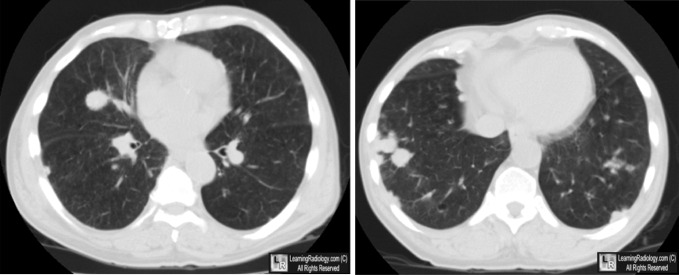
Rheumatoid Nodules. Above: Frontal radiograph of chest shows innumerable nodules scattered throughout both lungs (white arrows). Below: Two images from a CT scan of the chest show the nodules are mostly subpleural in location (yellow arrows). Patient had a long-standing history of rheumatoid arthritis and nodules were unchanged for 6 years.
For these same photos, click here and here
For more information, click on the link if you see this icon 
Rheumatoid nodules: differential diagnosis and immunohistological findings. EM Veys and F De Keyser. Ann Rheum Dis. 1993 September; 52(9): 625–626.
Rheumatoid Arthritis–related Lung Diseases: CT Findings. Ni Tanaka, JS Kim, JD Newell, KK Brown, CD Cool, R Meehan, T Emoto, T Matsumoto and DA Lynch. July 2004 Radiology, 232, 81-91
|
|
|

{kind=link}
{kind=link}